EEHV Treatments
Treatment of Elephants with Elephant Endotheliotropic Herpesvirus Hemorrhagic Disease
Ellen Wiedner, V.M.D., Dipl. A.C.V.I.M. (Large Animal)
Updated 2019 by North American EEHV Advisory Group Veterinary and Management Resources Committee
General Introduction
Treatment protocols for EEHV Hemorrhagic Disease (EEHV HD) are derived from therapies used for the treatment of human hemorrhagic diseases. Like EEHV, these human diseases, which include Ebola and Marburg, present initially with non-specific and often subtle signs. Also like EEHV, these diseases progress rapidly with death likely resulting from shock, hypovolemia, and possible disseminated intravascular coagulation (DIC), but not from blood loss, per se, although anemia and thrombocytopenia can be substantial.
The goal of therapy with human hemorrhagic diseases is to provide supportive care and to maintain tissue and organ perfusion. This is also the goal of EEHV treatment. Circulatory support and maintenance of blood volume require aggressive fluid therapy using crystalloids, colloids and sometimes both, in conjunction with an intensive care approach to monitoring the patient and symptomatic treatment. Although antiviral drugs are used for EEHV, their actual role in fighting disease is controversial and as yet unconfirmed.
Logistics of providing medical care to sick young animals
Logistics of providing medical care to sick young animals
Elephants need to be trained to accept medical procedures. Calf training should be started immediately after birth with the youngster being taught to stand still and tolerate being touched, and over time, progressing to having blood drawn, allowing intramuscular and intravenous injections, swallowing oral medication, and receiving rectal fluids. If the calf has not been trained, then sedation will be needed so that medical care can be given. All sick elephants must be provided with appropriate medical treatment when in human care. Facilities that are breeding should make calf training a priority, but any facility with elephants should accustom their animals to routine medical care so that sedation, always tricky, but riskier in sick animals, isn’t necessary.
Courses on training elephants are available in the United States and Europe through various organizations. Calf training is discussed here: Minimum standards of elephant care.
Strategic planning is needed for the eventuality of an EEHV-HD case. Some facilities in the United States perform preparatory drills where the supplies are checked and confirmed (adequate amounts, not expired, properly stored, etc), the elephants’ training levels are reassessed, phone tree numbers are checked and so on. A team approach is critical for these cases; thus the head of the facility, the public relations coordinator, and even neighboring institutions that could lend moral or physical support should be included in the preparation
Because elephants with EEHV usually need round-the-clock care, facilities should determine how to provide such staffing well in advance of an actual emergency. Facilities should also have a budget for medications and equipment, and should keep adequate amounts of supplies on hand, as well as basic laboratory equipment that can be kept near or in the elephant barn. Because care for EEHV-HD affected elephants is performed in the barn – not in a hospital — facilities need to be able to turn the barn into an intensive care unit (ICU). Recommended supplies for an elephant ICU are listed in Table 1.
Table 1: Supplies for the Elephant Barn
- Easily cleanable table for storing supplies
- Sharps container
- Red top and purple top and blue top (for blood clotting evaluation) vacutainer tubes (Note Activated Clotting Time tubes are not useful in elephants)
- Plasma collection bags and plasma press (plasma extractor tool)
- Styrofoam containers
- Microhematocrit tubes and clay
- Microhematocrit tube centrifuge
- Microhematocrit PCV chart
- Oxygen tank (E-tank) on a portable stand with wheels and tubing to provide intranasal oxygen
- Ophthalmoscope
- Stethoscope
- Thermometer
- Pulse Oximeter
- Glucometer and glucose sticks
- Urinalysis strips
- Refractometer (serum protein measurement)
- Light Microscope
- Glass microscope slides
- Needles and syringes
- Small refrigerator for medication and blood tube storage
- Record keeping supplies (notebook and paper, computer access etc)
- Blood pressure cuff and blood pressure reader
- Good quality flashlight
- Soft rubber tubing for administering rectal fluids
- Large equine dosing syringe to attach to tubing
- Equine stomach pump and a large metal bucket for administering fluids
- Handwashing supplies
- Develop a emergency drug box and emergency drug chart
- Gloves for personnel
Fluid Therapy for Confirmed EEHV cases
The first line of treatment is rectal fluids. Plain water administered through a garden hose or through rubber tubing via an equine gastric pump can be lifesaving for these animals. This is fortunate for the clinician because administering copious quantities of rectal fluids is straight-forward and appears to be very safe. The elephant colon is extremely absorptive, and elephants will absorb what they need while excreting the rest. To administer rectal fluids, the animal should be restrained in a chute. The hind legs may need to be tethered. Manual evacuation of manure is done expediently; it is important not to irritate the colon which will increase peristaltic activity and cause the fluid to be expelled before it is absorbed. Next, the hose (with all metal parts removed) or soft rubber tubing (such as an equine nasogastric tube) should be lightly lubricated and pushed into the rectum to the length of the clinician elbow. The clinician should then withdraw the arm and hold the tail down to encourage fluid retention. (use of electrolyte solution with rectal fluids may be warranted).
Lukewarm rectal fluids should be administered a slow steady rate. Too fast, and the fluid will stimulate peristaltic contractions, which is not desirable. At the end of fluid administration, the tubing should be swiftly withdrawn and the elephant’s tail held down for about a minute. If the animals starts to strain at any point, the fluid should be turned off but the hose left in place until the straining stops. The fluid should then be started at a somewhat slower rate.
Fluid rates and doses are empirical. A bolus technique of 10 to 20 ml/kg dose is often used. Most elephants will show immediate improvement after receiving fluids. Fluids often need to be given hourly or every two hours. However, it is important to be gentle because it is possible to damage rectal mucosa. If the clinician’s glove comes away with blood on it, this indicates rectal irritation. Fluids should be continued, but additional lubrication and more care should be used.
If the elephant doesn’t show improvement with rectal fluids, or bloodwork and physical exam indicate the animal’s condition is deteriorating, i.e. tachycardia, tachypnea, increased depression and lethargy, intravenous fluids can be added to the regime. Asian elephants have very low serum osmolarity and are hyponatremic and hypochloremic compared to other species. African elephants are thought to have similarly low serum osmolarity. Thus, commercial fluids such as Plasmalyte, Norm-R and similar, are actually hypertonic for elephants. Hypertonic fluids should be administered in very small amounts; (1 liter per 1000 lbs; 1 liter per 450 kg) may be given through an IV catheter and followed afterwards with large amounts of rectal fluids.
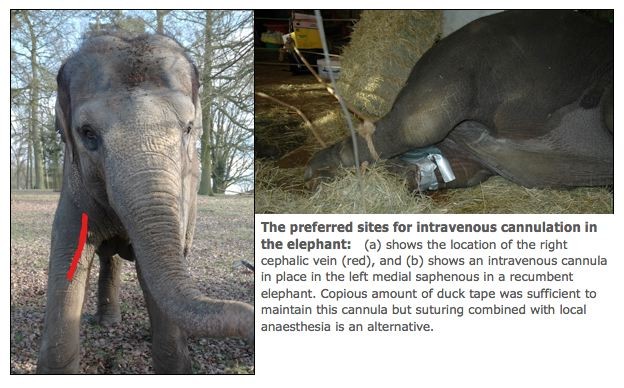
Colloids may be needed as well, and small amounts can be extremely helpful. Plasma or blood can be banked and stored or collected fresh from another elephant. It is important to make sure that the donor elephant is not viremic and is in good health. In addition, because elephants have preformed blood group antigens, crossmatching in advance of a transfusion is essential. Blood and plasma should be administered through an appropriate blood filter to prevent clots. Very small amounts of plasma, 2-4 liters per elephant, have been quite beneficial for sick elephants. One possibility is the administration of a loading dose of antiviral medication to the plasma donor and blood collected about 1.5 hours after administration. Another strategy would be to administer a loading dose of antiviral medication to a potential donor prior to its expiration date and the resultant plasma frozen and stored for future use. Colloids must be administered through an intravenous catheter. Catheters can be placed in an ear or saphenous vein. Aseptic technique should be used to place the catheter. After fluid administration is completed, the catheter should be pulled and adequate pressure placed on the insertion site to prevent hematoma formation. Leaving the catheter isn’t recommended in elephants because they will remove or damage it.
Antiviral Therapy
EEHV is such a peculiar virus that it is unclear at this time what drug is best to combat it. Famciclovir is most commonly used and can be administered orally or rectally. Acyclovir, which can be given orally and gancyclovir which requires intravenous administration, have also been used. Most facilities use famciclovir rectally because compliance is straight-forward and no side effects are reported with its use. Gancyclovir is associated with severe side effects in other species including bone marrow suppression and development of Fanconi’s syndrome. To date, such side effects have not been noted with use in elephants. If a side effect is noted, it should be reported to the FDA and an EEHV Advisorycommittee member.
If famciclovir is administered rectally, it should not be given at the same time as rectal fluids. Ideally, famciclovir would be administered first, and then at least an hour allowed to pass before rectal fluids are given. As with administration of fluids, retention of rectal medication requires not overly stimulating the rectum and causing the drug’s expulsion. Famciclovir tablets can be dissolved in warm water and the solution placed in a dosing syringe. The syringe can be attached to a soft rubber tube (equine nasogastric tube), and the tube inserted into the rectum as for fluid, following removal of manure by hand.
While there is no clear evidence that famciclovir is an ideal drug to fight EEHV-HD, its safety and the possibility that it does help suggest that clinicians should continue to use it. Suggested doses can be found in Table 2.
Table 2: Drug doses for elephants with EEHV-HD”
| Drug | Dose | Frequency | Route | Notes |
|---|---|---|---|---|
| Butorphanol | 0.01-0.03 mg/kg | Q 4 hours | SQ, IM or IV | Can be given more frequently if necessary; an appropriate dose should not make the elephant overly sleepy |
| Ceftiofur | 1.1 mg/kg | IM or IV | Twice daily; Once daily if IV | Can cause abscess formation given IM |
| Flunixin meglumine | 0.2 – 0.5 mg/kg | IV | Once a day | Animal must be adequately hydrated first. Intramuscular administration is extremely necrotizing to tissue |
| Famciclovir | 16 mg/kg for one day then 12 mg/kg | Oral or per rectum | Four times/day | |
| Acyclovir | 15 mg/kg | Oral or per rectum mostly. Intravenous option is possible | Twice a day | Grind with mortar and pestle, mix with water until paste consistency, then further dilute with water |
| Ganciclovir | 5 mg/kg | Intravenous | Twice a day | SLOW iv via IV catheter. Dilute in 1 liter of fluids, given over one hour |
| Sulfa-trimethoprim | 22 mg/kg | Oral | Twice daily | |
| Vitamin E | 2.2 IU/kg | Oral | Once daily | Used as an antioxidant |
| Butorphanol plus detomidine | B: 0.02 – 0.03 mg/kg; D: 0.02-0.03 mg/kg | IM | Given in one syringe for sedation | Reverse Butorphanol with naltrexone at 5 mg per 1 mg opioid (optional); Reverse Detomidine w atipamzeole at 0.1 – 0.16 mg/kg |
| Omeprazole | 1 mg/kg (prophylaxis); 4 mg/kg (treatment) | Oral | Once daily | |
| Vitamin C | 30-50 mg/kg | Oral | Once daily | May be given IV slowly diluted in one liter of fluids |
| Dexamethasone | 0.05-0.5 mg/kg | IM or IV | ONCE | May be considered. Efficacy is controversial. SINGLE dose only |
Other therapy
Prophylactic antibiotics, anti-inflammatories, H-2 blockers, and other drugs are often used in elephants with EEHV-HD. Doses can be found in Table 2.
Monitoring of Confirmed EEHV cases
Monitoring should be done frequently; in some cases hourly as critical parameters change. Watching the hematocrit for progressing anemia and thrombocytopenia is very important. This can be done using a microhematocrit tube so that minimal blood is required, and results can be obtained stallside. A light microscope and H&E stain can be used to evaluate the blood smear. The increase or decrease in reactive white blood cells, band heterophils and/or cellular toxicity in the cells can be prognostic. Temperature, pulse, and respiration (both rate and effort) should be measured. Assessing mentation and somnolence are important because changes can indicate electrolyte disturbances, hypoxia or brain bleeds. Decreased urine output and scant feces can indicate an animal that requires more fluids. Pain can be a component of the disease, evidenced as colic, oral ulcerations or lameness, and requires treatment. Sick juvenile elephants should be weighed regularly (daily) understanding that there may be daily physiologic fluctuations in weights and margins of error expected from the scales that may affect accurate assessments.
Measuring oxygen saturation of hemoglobin with a pulse oximeter on the tongue is important in more severe cases. The heart should be ausculted in elephants weighing less than 4500 lb (2000 kg) by placing the stethescope just caudal to the elbow, and then as far under the elbow as possible. The presence of tachycardia or heart murmurs can indicate progressing disease. Difficulty hearing the heart raises concern about pericardial effusion; this can be confirmed with a gel-covered ultrasound transducer placed over skin that has been thoroughly soaked first with water. Changes in the color of the mucus membranes, particularly a cyanotic color, are concerning. These animals may benefit from nasal oxygen supplementation.
Some elephants show evidence of hepatopathy by ultrasound, development of lipemic serum, or liver enzyme changes in the SBC. Adding Vitamin E, an antioxidant, may be helpful.
Recumbent elephants should have adequate padding under them, and should be turned regularly. Prognosis declines for animals too weak or sick to get up without assistance.
Recommended references:
Hall NH, Isaza R, Hall J, S., et al. Serum osmolality and effects of water deprivation in captive Asian elephants (Elephas maximus). Journal of veterinary diagnostic investigation 2012;24:688-695.
Howard LL, Schaftenaar W.. Elephant endotheliotrophic herpesvirus (EEHV). In: Miller, RE, N Lamberski and P Calle (eds) Fowler’s Zoo and Wild Animal Medicine Current Therapy, 9th ed: 672-679, 2018.
Isaza R, Hunter RP, Richman LK, et al. Famciclovir pharmacokinetics in young Asian elephants (Elephas maximus). American Association of zoo veterinarians 2003;82.
Weber M, Junge R, Black P, et al. Management of critical juvenile Asian elephants (Elephas maximus). Proceedings of the AAZV 2009:82-83.
Wiedner E, Hale A. Evidence of specific blood types in Asian elephants (Elephas maximus) and significant incidence of positive crossmatch. Proceedings of the AAZV and AAWV joint conference 2010:173.
Wiedner E, Howard LL, Isaza R. Treatment of Elephant endotheliotropic herpesvirus (EEHV) In: Fowler ME,Miller RE, eds. Fowler’s Zoo and Wildlife Medicine 7 Current Therapy: Saunders, 2012.